Epidemic Urbanism: Contagious Diseases in Global Cities
Part 4: Urban Design And Planning: Interventions and Implications
Case studies presented:
- Chapter30: Public Health, Urban Development, and Cholera in Tokyo, Japan, 1877-95
- Chapter31: The Hong Kong Plague and Public Parks in the British Settlements of Shanghai and Tianjin, China, 1894
- Chapter35: Urban Transformation and Public Hearth Policies in Post-Influenza Lagos, Nigeria, 1918
Date presented: 26th June 2023
Presenter: Kazuki Hirabayashi
Chapter30: Public Health, Urban Development, and Cholera in Tokyo, Japan, 1877-95
In the late 19th century, Japan experienced a devastating cholera epidemic that claimed the lives of over 360,000 people across the country, with Tokyo being severely affected. Tokyo accounted for more than 11% of all cases, despite its population representing only 3.2% of the total population. The government’s objective was to comprehend the factors contributing to the spread of cholera in the city and develop policies for disease control.
Cholera is caused by Vibrio cholerae, a comma-shaped bacterium that originated in the warm waters of the Ganges Delta. Poor hygiene and inadequate sanitation practices facilitate the contamination or recontamination of water, serving as a vector for the widespread and easy transmission of the disease. Despite the detrimental role played by an aging water system and insufficient sanitation in the disease’s spread, the government was slow to take action in improving the city’s infrastructure.
The infection rate was particularly high in wards with dense populations and significant water pollution. In 1854, the British physician John Snow demonstrated that cholera spreads through water contaminated by human waste, and by 1871, this knowledge had reached Japan. This understanding reinforced growing concerns about drinking water and sanitation in Tokyo.
During the latter half of the 19th century, Tokyo continued to rely on an outdated water system established in the mid-17th century, namely the Kanda Waterworks and Tamagawa Waterworks. These waterworks supplied water that was heavily contaminated with organic matter due to waste flowing through canals and underground pipes throughout the city. However, due to the high costs involved in improving the water supply system, no significant improvements were possible without funding from the central government.
As the Japanese government prioritized military and industrial spending, Tokyo’s public health authorities responded to cholera by implementing restrictions on the daily activities of residents. These measures included addressing the manure trade, restricting waste collection and removal to nighttime, requiring waste buckets to be covered, replacing toilets with ceramic ones, regularly cleaning drains, roads, and garbage dumps, and prohibiting urination and washing clothes or dishes near public wells.
Another strategy involved isolating infected individuals in quarantine hospitals. By 1889, an improved system of “infectious disease hospitals” had emerged, but they were often located on the outskirts of the city, reflecting discrimination against the infected. Quarantine hospitals predominantly targeted poor and working-class residents, which fostered popular hostility towards the patients.
In conclusion, despite studies revealing the contamination of Tokyo’s water supply, little effort was made to address the underlying infrastructure issue. Instead, the government focused on regulating the behavior of urban residents to prevent the spread of the disease. This situation highlighted the social, economic, and material inequalities that influenced urban life, with working-class residents lacking access to clean water and sanitation and sometimes being forcibly transferred to isolation hospitals.
Chapter31: The Hong Kong Plague and Public Parks in the British Settlements of Shanghai and Tianjin, China, 1894
In 1894, the plague was spreading in Hong Kong, and the British settlements of Shanghai and Tianjin had strong trade connections with Hong Kong. British settlers in these settlements implemented their urban planning concepts and responded to the plague by importing public health and infrastructure ideas from Europe, including the creation of public parks.
Following the outbreak of the plague in Hong Kong, it was believed that parks could serve as a means to prevent diseases (as the British attributed diseases to the environment). Urban authorities utilized parks to promote changes in social practices that could endanger public health. For instance, in Chinese cities at the time, urine was commonly dumped directly into the streets, so lavatories were constructed in parks to address this issue.
In Shanghai, a public water system was introduced in 1883, and in Tianjin in 1898, aiming to enhance public health. As part of these improvements, public water fountains were installed in parks. Lavatories and water fountains gradually became standard features, and the overall design of public parks was enhanced. Public parks came to be recognized as crucial elements in maintaining public health and welfare.
During the early 20th century, with the extensive expansion of new urban developments, there were concerns among residents about the potential reoccurrence of the plague. In response, city councils actively promoted the construction of public parks in rapidly growing districts. In 1930, a European-style “park system” was introduced, ensuring that small parks were built within a certain distance from each resident’s residence.
In conclusion, British settlers brought European urban planning ideas to China through the establishment of parks. This included the introduction of lavatories and water fountains, gradually making parks an integral part of public health initiatives. Even after the plague epidemic subsided, the concept of a park system continued to influence urban planning and the lives of residents. Despite increasing land prices, small parks were constructed to improve the urban environment and provide ventilation.
Chapter35: Urban Transformation and Public Hearth Policies in Post-Influenza Lagos, Nigeria, 1918
The city of Lagos, situated on the southwestern tip of Nigeria, facing the Gulf of Guinea, served as the administrative center of the Nigerian government during the colonial period. It was annexed by the British Empire in 1861 and became a colony. The concentration of settlers in Lagos led to overcrowding, both in terms of sites and dwellings, which contributed to poor sanitary conditions.
The influenza epidemic of 1918-19 was one of the deadliest in history, claiming the lives of 50 to 100 million people worldwide. In Lagos, the lack of accurate information and the dissemination of misinformation by the colonial government facilitated the spread of the disease. Additionally, the colonial government prioritized its efforts towards World War I instead of focusing on combating the epidemic.
The colonial government estimated the number of deaths based on death registers maintained by local government offices. According to a 1918 report, an estimated 1.5% of the Lagos population succumbed to the disease, with a higher mortality rate observed among the poor and illiterate segments of society (Table 1).
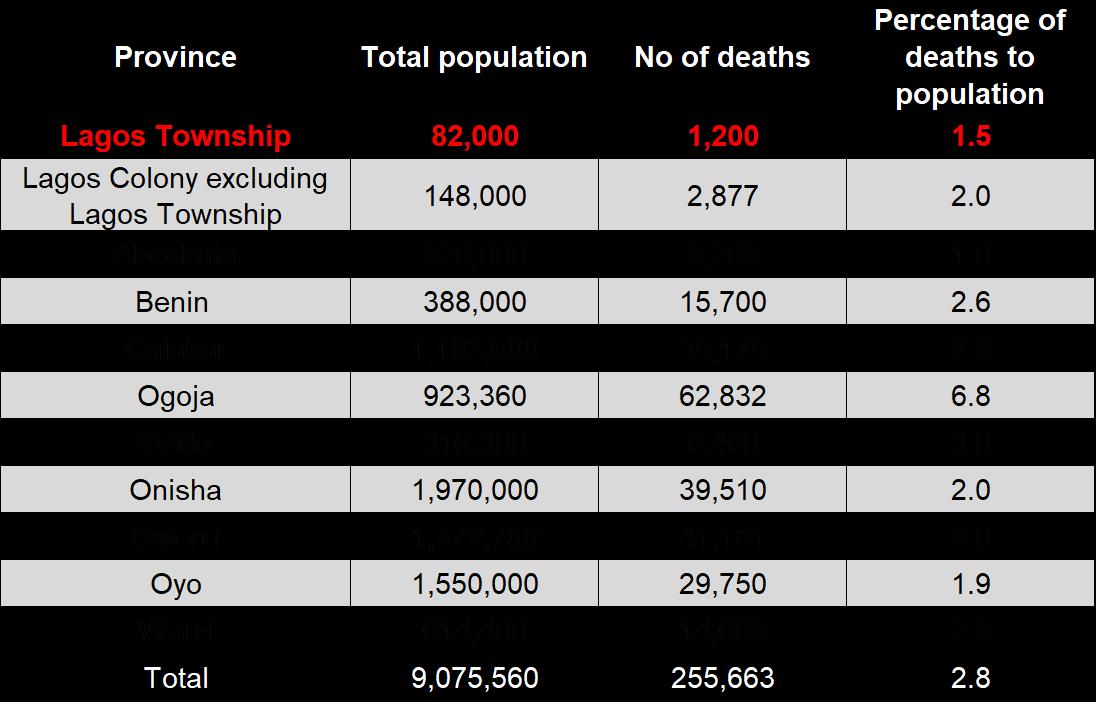
Table1: Death records of the colonial government in Lagos colony and other southern states between 1918-19
As a response to the influenza epidemic, schools, stores, and public places were closed. The authorities implemented sanitation reforms, including the introduction of piped water supply, urban planning measures, wetland reclamation, drainage improvements, and the enactment of public health ordinances and regulations. Medical and insurance services were also expanded, resulting in a significant increase in the number of medical staff. A network of local pharmacies staffed with indigenous doctors and nurses was established, and elementary hygiene education was provided in large town schools under the supervision of government officials.
Furthermore, various segregation schemes were implemented in the settlement, some of which still persist today. British settlers were segregated from the indigenous population into Government Reserves (GRA). The challenge of ensuring adequate housing and infrastructure for Nigeria’s people remains unresolved.
In conclusion, epidemics had a profound impact on Nigerian society and its built environment. Urban sanitation reforms were implemented only after the epidemic had already spread extensively. Although the pandemic could have been contained without government intervention, it would have taken longer and resulted in more infections and deaths. In Nigeria, the disease was largely left untreated, leading to a significant loss of life. However, significant progress has been made in implementing health measures in different regions of Nigeria.
Lesson learned
- Even in the midst of an epidemic, other policies may be prioritized over sanitation policies due to circumstances or funding difficulties. However, inadequate sanitation policies slow the control of infectious diseases and increase the number of victims.
- Epidemic outbreaks provide an opportunity to improve health services, infrastructure, and urban planning.
- Social and economic inequalities worsen the effects of epidemics. Therefore, ensuring equitable distribution of resources is important in promoting public health.
Discussion
- By drawing lessons from the history of epidemics, new public health measures can be incorporated into the system, and future occurrences of similar cases can be predicted.
- One reason why children may lack knowledge about public health is the absence of parental education on the subject. Therefore, including “hygiene education” in the school curriculum can aid in public health measures. Additionally, ensuring accessibility to soap and other hygiene products is crucial for emphasizing the importance of handwashing. Furthermore, adopting a more comprehensive approach, similar to the BOP (Bottom of the Pyramid) business model, can encompass easy access to sanitary products while considering the reduced environmental impact associated with their disposal.
- While public parks play a significant role in sanitation measures, facilities such as athletic fields, soccer fields, and tennis courts are also vital for promoting health by enabling people to participate in sports and physical activities. Regular physical activity strengthens the immune system and may help prevent infectious diseases.
- Community organizations are essential, particularly during epidemics when misinformation can circulate. In such situations, having a connected community and a reliable source of information, such as the government, can reduce confusion by facilitating the dissemination of accurate information within the community.
- Given the impact of public health on human resources, it should be a top priority when allocating government budgets. It is important to note that sanitation measures benefit a large number of citizens. However, in cities strongly influenced by those in power, the authorities may prioritize other policies based on their personal concerns. Unfortunately, significant decisions often tend to be made only in response to major events. In other words, progress is slow without a triggering event, whereas action is swift when a significant incident occurs.
Reference
Gharipour, M., & DeClercq, C. (Eds.). (2021). Epidemic Urbanism: Contagious Diseases in Global Cities. Intellect Book. pp.240-320.